
Jambo!
Our first full day at Lewa is finally here and we are really excited to get started. We begin with a hearty Kenyan breakfast of sausage, bacon, eggs, crepes, toast, roasted tomatoes, fruit and cereal. And lots of tea!
We headed to the clinic with Benjamin our main driver for the week. Our commute in is always incredible. The air, the animals, the sounds, the people walking along the roads….it all creates an atmosphere of reflection and gratitude for this opportunity to be here and to help this beautiful community.

We arrive to Rosaline, a complete force of nature. One of those people you hear before you see. Her energy could quite literally power a small city. I first met her some years ago now when she was cleaning floors at the clinic. Our autorefractor we brought with us to donate to Lewa had blown a fuse and we needed desperately to replace the fuse. She was the first to step in and offer to drive the 40 minutes into town to buy a new one. She quite honestly saved the day and I will never forget her big smile when she returned and proudly handed me the bag holding the new fuse. Since then I’ve seen her do any number of things at the clinic, including cleaning floors, carrying supplies, driving into town to run clinic errands, crowd control at outreaches…. anything that someone needs, she’s there for you. But what I most know her for is her enormous smile and incomparable, unconfined energy and excitement when we arrive at the clinic. When we arrived, she was hugging all of us, including the new team members, making us feel so welcome. She is truly special and we are so happy to see her. Later that day it is Rosaline who will prepare tea for everyone and pass it around personally to each person, tray with cups and sugar in one hand and a steaming thermos of milky tea in the other. Once again, spreading her magic and making everything just a little bit better.


The morning is spent conducting Continuing Medical Education to the staff by the doctors. Most of the presentations are by request of the staff based on medical topics they would like to learn more about. Today’s talks include:
- Dr. Michael – Integrated Management of Childhood Illness
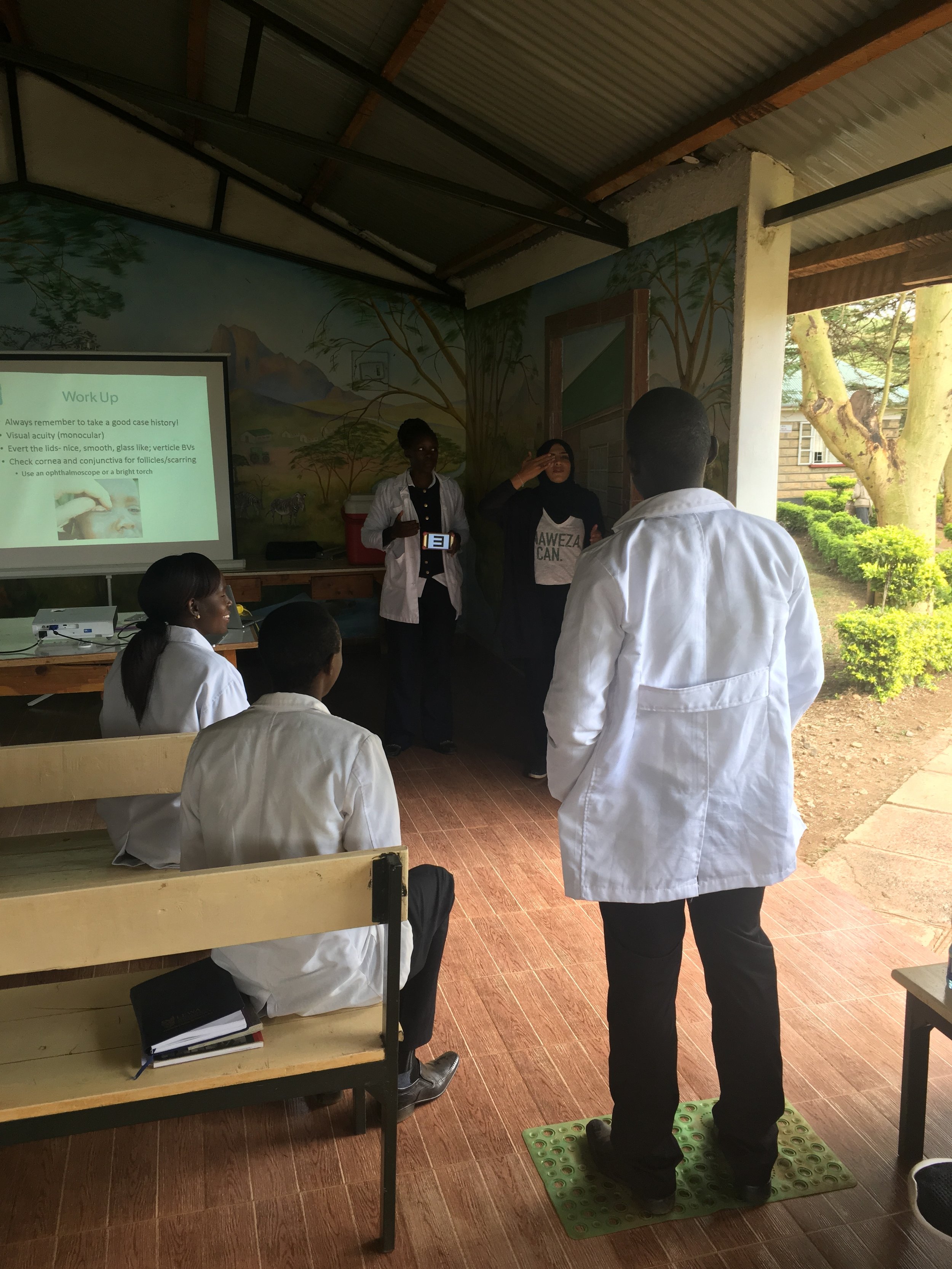
- Dr. Sidiqa – Trachoma (eye disease)
- Dr. Tanya – Sexually Transmitted Infection Prevention and Treatment
The doctors take more of an interactive approach to training. Combining case studies from Canada and Kenya, and questions from the clinicians have provided the best learning experience in the past. We want the staff to be an active part of the talk so that we understand the real-life situations that they encounter and the challenges that they are up against.





One of the best moments was when Dr. Sidiqa asked Lydia to get up in front of everyone and show how she performs a vision screening test on a patient. On the last trip Dr. Sidiqa provided Lydia with a “Vision Screening Kit” which includes:
- A vision chart (PEEK app on Lydia’s phone)
- Measuring tape to measure the distance from the chart to the patient
- A mat for the patient to stand on at 3m
- A bright torch and some batteries
- An Ophthalmic Emergency manual
- Naweza Stickers “I had my eyes screened today”
- Logbook and stationary
A typical Vision Screening uses two mobile apps.
- Using a smartphone-based vision check app called PEEK, Lydia shows the patient a visual acuity chart (the letter “E”) on her phone at 3m away. The patient is asked to point with their finger the direction of the letter “E” that they can see. Lydia then swipes her screen in the same direction as the patient. The E keeps getting smaller and smaller until the patient is no longer able to tell its direction. The app gives Lydia the final visual acuity of the patient which she then records on the second mobile app on her phone.
- Utilizing her phone once more, data such as patient’s name, age, school/area they’re from and the visual acuities are recorded on an online database called KoboCollect. Lydia analyzes the patient’s visual acuities from the PEEK app and records the results as “pass” or “fail”. Any patient that does not pass the vision screening is then referred on to our local optometrist visiting Lewa once a month.
Lydia loves being able to use her mobile phone to do the vision screening as well being able to record the results online! This also allows Dr. Sidiqa to be able to remotely follow the process of the screening and review the data.

After returning to Ngiri House for a delicious lunch, Dr. Michael, Jen and I visited John Kinoti at Lewa’s offices to discuss the future of our relationship with Lewa. For the last 6 years we’ve been coming to Lewa and working with the clinic, providing education and training to the staff. All of the programs that we’ve done have been based on mutual trust by both parties. And it has worked very well so far. But we both feel it’s time to formalize the relationship as we’ve reached a point of bigger potential. Our goal is to make Lewa a “Centre of Excellence for Chronic Disease Prevention and Treatment.” Our framework includes:
- A Community Health Worker (CHW) screening communities using SMS technology
- EMR system managing treatment and compliance of Chronic Disease patients
- Training and education of the clinic staff
- Data collection to conduct research studies to ensure program effectiveness
With early detection and proper treatment management, we believe that health outcomes will improve for the Lewa community.
While we met with John, Dr. Tanya, Dr. Sidiqa and Kristen went to the clinic and saw patients. They worked alongside the nurses and provided real time training. The process they follow is:
- Lewa nurse obtains a history of the patient and communicates it to the Naweza doctor
- Lewa nurse performs a clinical examination with the Naweza doctor providing guidance
- Naweza doctor asks the Lewa nurse for their opinion on the diagnosis
- Naweza doctor and Lewa nurse discuss, providing an opportunity for the doctor to train and educate
It’s important that the Lewa nurse still “owns” the patient and that the Naweza doctor is simply there to provide guidance. We are only here twice a year and if our doctor makes all decisions with regard to the patient, we will have not prepared the Lewa clinicians as well as we could have. The goal is that when we leave, the nurses are able to provide a higher level of care to their community. We also want to build confidence in the community by showing that we believe in their nurses to take care of them and provide quality healthcare. And as I’ve mentioned in past blogs, the Lewa Clinic has access to a doctor once or twice a month. But the clinic cares for many patients a week who sometimes suffer from complex conditions that would be handled by a doctor if they were in Canada. But in this resource-limited setting, the nurses are expected to step in as the “doctor.” A very big expectation and a lot of pressure for the staff! So we try to give them training, education and technological tools to help them manage these complex cases and hopefully improve the level of care provided to their community.
That’s all for now. Thanks for reading!
Stacy ☺
