Jambo!
It’s hard to believe, but it is in fact our last full day at the hospital. It has been an incredibly productive visit with our new friends at Kambuga and we feel optimistic we can develop a program here that will benefit them.
We started the day with Dr. Rajiv doing a surgery in the OR with Vanessa and Dr. James as assistants, along with the other staff at the hospital. He removed a man’s enlarged prostate and was able to provide valuable training and insight on the procedure.

Dr. Michael did rounds in the pediatric ward. Very sadly a young 3 month old baby girl came in presenting with incessant cough and irritability. The diagnosis was whooping cough. The baby had 2 out of 3 of the required vaccinations, but with the vaccinations being incomplete she was at risk of contracting the disease. Dr. Michael measured her oxygen saturation and determined that the baby needed oxygen. Fortunately for the community in Kambuga, Dr. Michael has developed a technology that uses solar panels to power a condenser, turning air into pure oxygen. The solar panels also charge batteries so the condenser can be used at night. This allows the hospital to provide life-saving oxygen even when there are disruptions in the electricity, which is frequent.

Solar panels installed on top of one of the buildings at the hospital. The panels provide energy to deliver oxygen to the patients.
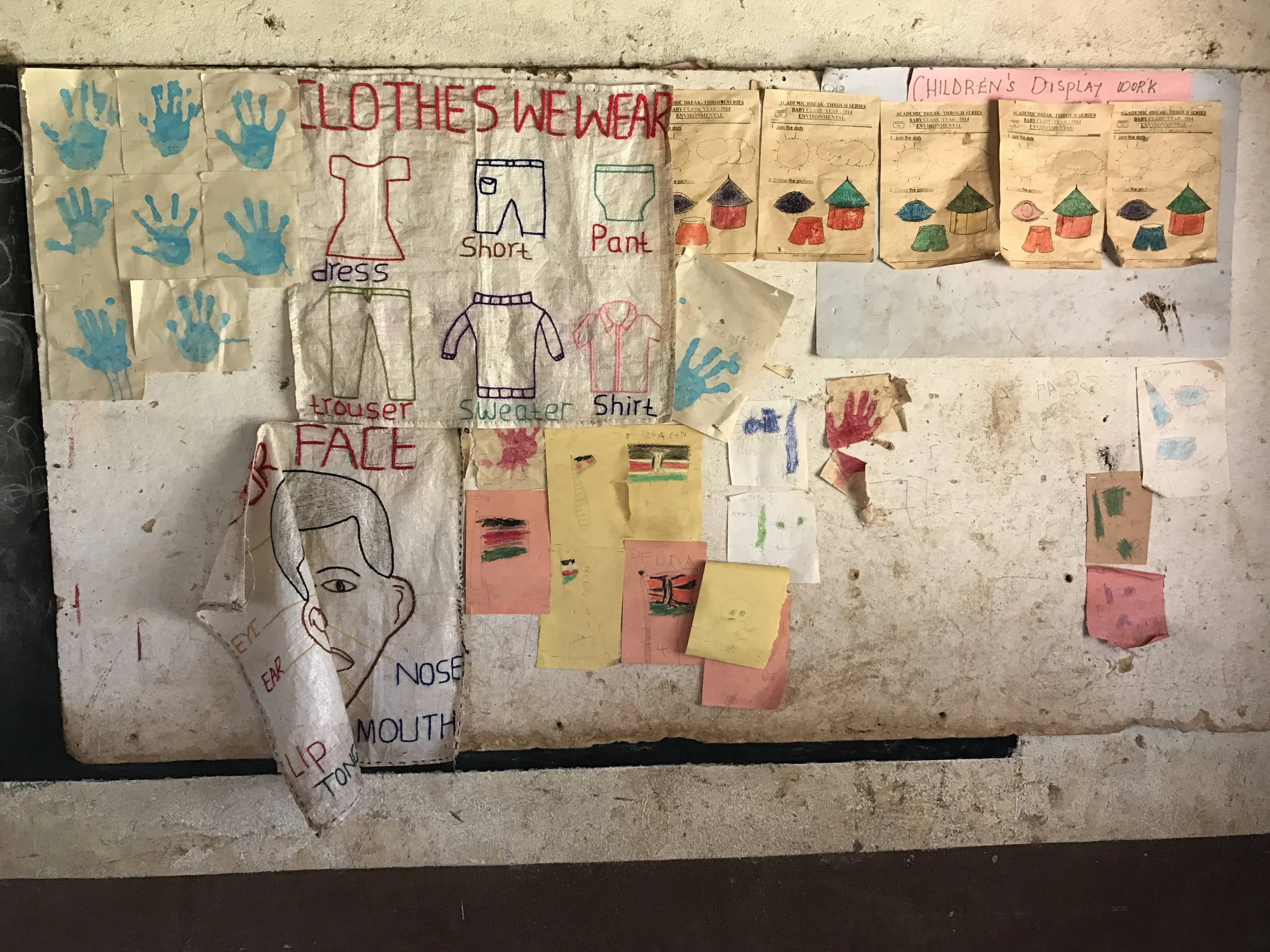
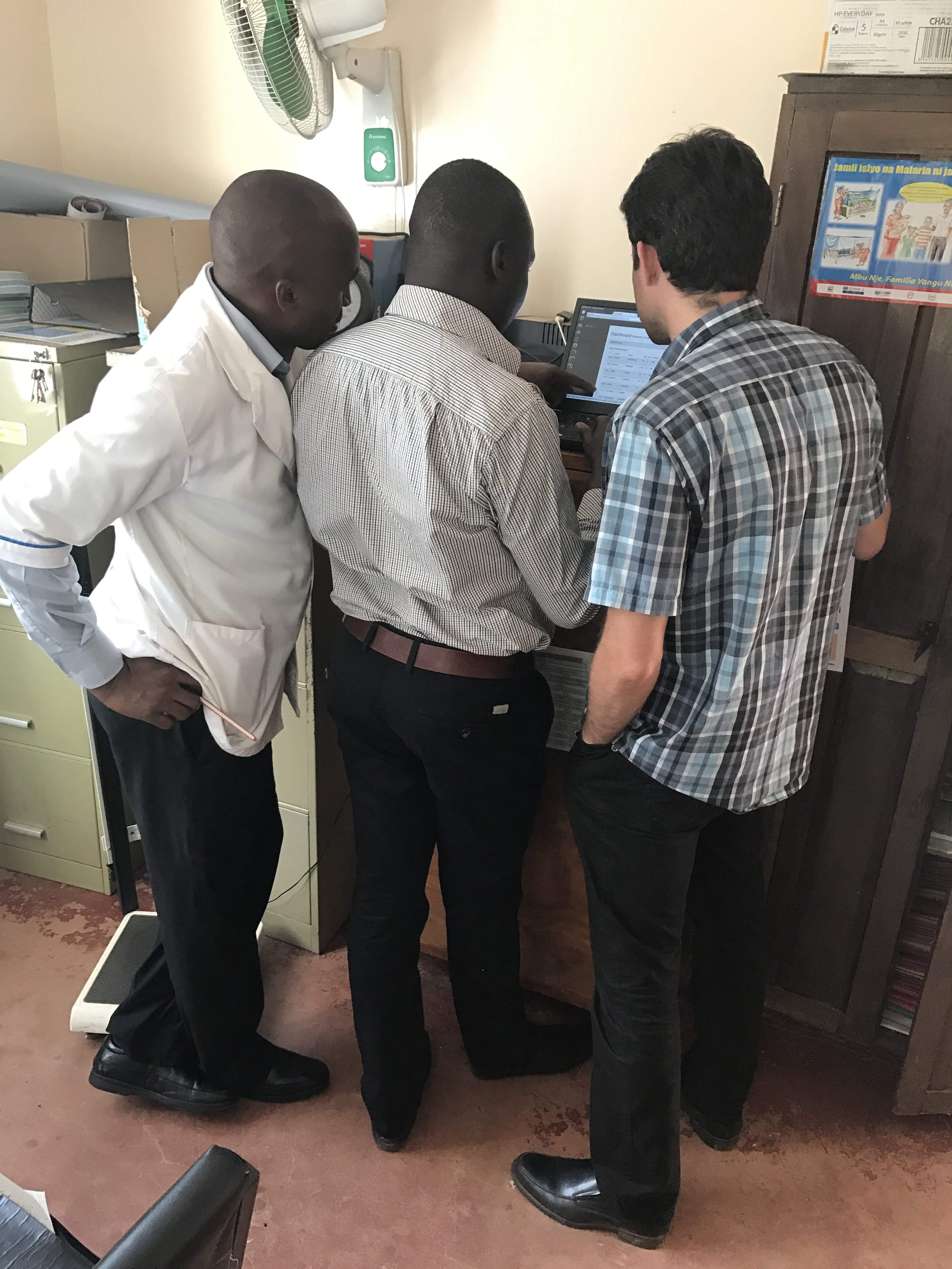
Dr. Sidiqa continued her training with Alex on the vision program. She is really happy with his eager to learn attitude and high level of ability. We only have so much time here, so it’s important to work with people that not only have the ability to learn, but the desire. Alex seems to have both. One of their patients was a burn victim. Hot milk spilled on his face five years ago leaving him with scarring on one side of his face affecting the eye as well. Fortunately he is able to see out of the eye, but he is unable to completely close his lid which causes many complications and increases his risk of infection. Dr. Sidiqa educates him on how to minimize the potential problems and discusses the issues with Alex as well so that he can continue to help the patient even after she leaves.
Dr. Michael also saw chronic disease patients in the outpatient ward. Based on the ability of the clinician he was working with and the medical records for these patients, he determined the hospital could benefit from some additional training. Our plan is to include education around chronic disease protocols in our program at the hospital.

A chronic disease patient having his blood pressure taken.

Dr. Michael working with a nurse at the hospital while seeing a chronic disease patient.
For dinner we were invited to the home of John, who is an employee of Dr. Michael's here in Uganda and is the person who helped organize the Ugandan portion of our trip. It was a traditional Ugandan dinner prepared by 6 women. It was an impressive display of local food and I can only imagine a tremendous amount of work. The dinner included home grown vegetables such as cabbage, pumpkin, plantains and potatoes as well as meat stew and different soups. And of course the delicious pineapple and watermelon for dessert. Simply perfect. They were so gracious and kind and our group was immensely grateful to have been invited into their home.

A small part of all of the delicious dishes we were served!

Dr. James and Dr. Rajiv with our host, John's father.
After 11 flights in 10 days, our trip has finally come to an end. We as a group feel like we’ve made considerable process on our initiatives and have even more ideas on how we can make an impact.
Once again, it has been a pleasure working with the members of the Naweza family. It is an incredible group and I’m so grateful for all of their hard work and commitment. Everyone who participates in this trip does so on a completely volunteer basis, taking precious vacation leave in order to come. Jen and Vanessa (my two “daughters” on the trip) are an absolute pleasure. Always happy and smiling no matter the challenge. Their contribution to Naweza is year long and not limited to just the trips to Africa. They layer their Naweza duties on top of their daily work schedule at Medcan, and I know put in a huge amount of extra time. We are very lucky to have them.
Dr. Sidiqa, my dear friend at this point, has been a dedicated and loyal member of the Naweza family. Out of 7 Naweza trips, she has been on 5 of them. The vision clinics that we offer during our time at the clinics have provided amazing stories of people who are now eternally grateful for the gift of sight. She works tirelessly during our time at the clinics and hospitals providing training and education to the staff so that they can continue to care for their patients after we leave. I am immensely grateful to have her as part of our team.
And a special thank you to Dr. Rajiv and his wife Sandra who were willing to take a chance and come to Uganda with us and help assess the potential of a Naweza relationship with this hospital. The unknown is always a bit daunting, and we as a team really had little idea of what to expect with this hospital. We worked through some challenging times together and I am sincerely thankful that they were there to provide valuable insight into how we could improve the standards practiced at the hospital.

Dr. Rajiv performing a prostate removal surgery and providing education and training to the hospital staff.
Dr. Rajiv taught a CME to the staff on catheters as well as promoted themes around surgical safety procedures and streamlining pre-op care using a patient safety checklist. Most impressively, he performed multiple surgeries including a prostate removal as well as various pediatric urological procedures. These patients won the lottery of sorts as not only were they able to have their surgeries done at no cost, but the surgeries were performed by a surgeon of Dr. Rajiv’s caliber. I am sure they each feel incredibly blessed.
With Dr. Rajiv’s feedback, one of our ideas is to layer on to our SMS technology tool a screening test for prostate cancer which would be conducted by the Community Health Worker out in the field. Prostate cancer is one of the leading causes of cancer deaths in Africa. The goal would be to do screening in order to identify those at higher risk of developing cancer. We would then bring a urologist with us once a year in order to do prostrate removal surgeries on those patients who do not have the financial means to pay for it themselves.
And a final big thank you to Dr. James and Dr. Michael, my fellow founding partners of Naweza. I feel very lucky to work with people who are at the top of their profession and who not only want to do something good in the world but want to have a good time doing it. We laugh our way through it all and with this spirit we have persevered since 2013 enduring many many challenges. But here we are now, beginning our own foundation with an innovative screening technology which enables Africans to identify conditions they are at risk for before that condition declares itself, thus resulting in better outcomes. There are countless applications for this technology, but our main focus at the moment remains screening for chronic disease. Our next step will be the Electronic Medical Record (EMR) which will allow the Community Health Workers and clinic/hospital to follow-up with those who have been identified as “at risk” in order to ensure that the patient is complying with their treatment strategy. Our goal is to have this ready by our next trip. Very exciting!

So, that’s a wrap! On behalf of the Naweza team, thank you for reading and for all of your support. Our next trip is planned for May 14th to 24th. So until then, make sure to keep following us on Instagram, Twitter and Facebook for updates on our programs. And we will continue to post photos from the trip throughout the year. We literally have hundreds and maybe thousands! Every moment is one you want to capture and remember always. We will be sure to share them with you!


Our final charter flight back to Nairobi. Everyone passed out, except for (I hope) the pilots! Thanks for all of the hard work team! You have about 4 months to recover until the next one!
Keep well and best wishes,
Stacy